Cáncer avanzado de recto bajo.
Resección anterior de recto ultrabaja transesfintérica TaTME + prostatectomía en bloque
Marcelo Viola, Diego Abreu, Diego Lapiedra, Alejandra Liz, Emilia Cerchiari, Juan Escuder, Gonzalo Gayo, Álvaro Lavega, Isabel Gabito, Andrés Schreiber
Unidad de Coloproctología, Clínica Quirúrgica “1”, Hospital Pasteur. Prof. Dr. Fernando González Calcagno. Montevideo, Uruguay.
Marcelo Viola
mviolam@gmail.com
Los autores declaran ausencia de conflictos de interés.
ORCID:
Alvaro Lavega: 0000-0002-0993-6847
Emilia Cerchiari: 0000-0002-4619-829X
Isabel Gabito: 0000-0002-1096-7982
Alejandra Liz: 0000-0002-1530-4782
Lucía Perez: 0000-0002-8709-1472
Diego Lapiedra: 0000-0002-1209-1697
Gonzalo Gayo: 0000-0002-3931-6403
Marcelo Viola: 0000-0003-2733-5276
Diego Abreu: 0000-0001-8232-5092
Juan Escuder: 0000-0002-7386-7559
Andrés Schreiber: 0000-0003-3239-7818
Recibido: diciembre de 2020. Aceptado: febrero de 2021.
RESUMEN
Introducción: El cáncer de recto bajo requiere un enfoque multimodal y multidisciplinario para su tratamiento. Hoy en día, la radioquimioterapia neoadyuvante es el tratamiento inicial, seguido de cirugía con intención curativa.
Es excepcional su presentación en edades tempranas, así como el compromiso de las vesículas seminales y la próstata.
Cuando existe infiltración prostática y de las vesículas seminales, la cirugía de elección es la exenteración pelviana. Pero, en algunos casos seleccionados, es recomendable realizar una cirugía de resección en bloque, preservando el aparato esfinteriano y la vejiga. Lo cual redundará en una mejor calidad de vida del paciente sin comprometer el pronóstico oncológico.
La anastomosis coloanal podrá realizarse en el mismo momento y protegerla con una ostomía, o en diferido mediante el procedimiento de pull through.
Descripción: Presentamos el caso clínico de un hombre de 24 años, con una historia de 3 meses de evolución dada por rectorragias, constipación y dolor pelviano.
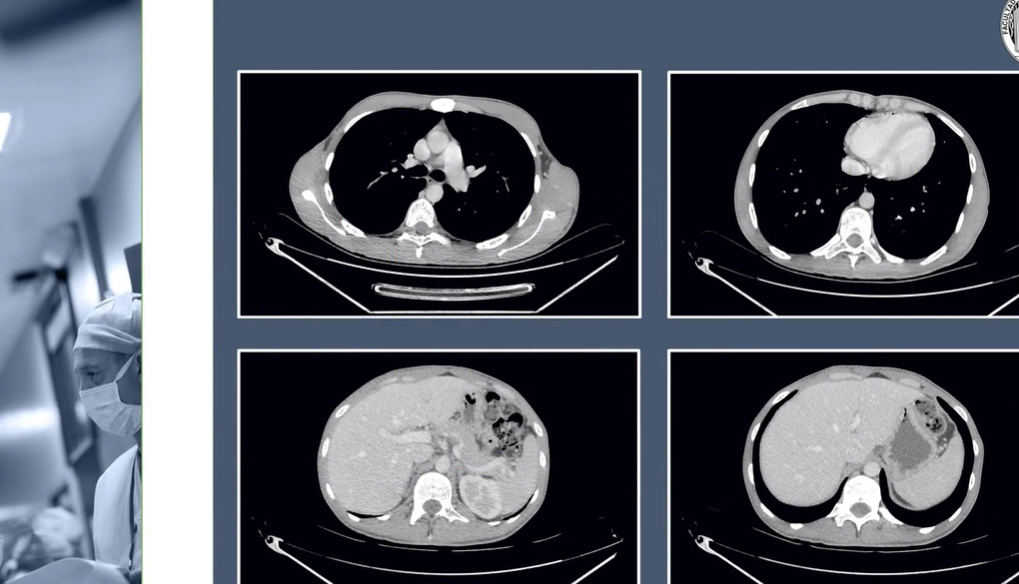
Se diagnosticó un cáncer de recto bajo con infiltración próstaticoseminal sin evasión sistémica. Se realizó neoadyuvancia con radioquimioterapia.
Se decidió en el comité de tumores, realizar una resección anterior de recto ultrabaja transesfintérica TaTME, más resección en block de la próstata y vesículas seminales por laparoscopía.
El paciente se colocó en decúbito dorsal, posición de Lloyd Davies, Trendelemburg 30º y lateralizado a derecha. Neumoperitoneo 12 mmHg con trocar óptico supraumbilical de 12 mm para la cámara. Se colocaron otros cuatro puertos, dos de 12 mm en flanco y FID para el cirujano, y dos de 5 mm en flanco y FII para el segundo ayudante. Se movilizó el ángulo izquierdo por abordaje medial; sección de la VMI por debajo del páncreas, y de la AMI en su origen. Completamos la disección retrorrectal, y por delante el sector ánteroproximal de las vesículas seminales.
El tiempo transanal comenzó por la disección interesfintérica hasta superar el anillo anorrectal, completando la ETM por vía transanal videoasistida. Simultáneamente, el equipo de Urología realizó la prostatectomía y liberación de las vesículas seminales en block con el recto, y confeccionó la anastomosis vesicouretral.
Se exteriorizó en forma de pull through el colon descendente. A 10 días se resecó el colon redundante y se aseguró la anastomosis coloanal.
El paciente cursó un postoperatorio sin complicaciones, tolerando vía oral con dieta progresiva, orinando sin sonda y movilizando el intestino. Se le dio el alta a 14 días de la cirugía inicial. Se controló a los 15 y 30 días estando asintomático, con continencia urinaria prácticamente normal. En la inspección perianal se objetiva un ano con pliegues mucocutáneos conservados y, al tacto rectal, esfínter algo hipotónico, que se contrae voluntariamente, logrando una continencia parcial.
Conclusiones: El cáncer de recto bajo localmente avanzado sigue siendo un desafío terapéutico.
La exenteración pelviana es la cirugía de elección para los tumores de recto con invasión genitourinaria. La cirugía de preservación esfinteriana y vesical surge como posibilidad terapéutica en casos estrictamente seleccionados.
La anastomosis coloanal diferida pull through ha resurgido en los últimos años con la finalidad de disminuir la necesidad de ostomas de detransitación y la falla de sutura.
Palabras claves: Cáncer de recto; Resección anterior ultrabaja transesfintérica; TaTME; Prostatectomía
ABSTRACT
Introduction: Lower rectal cancer requires a multidisciplinary multimodal approach to its treatment. Today neoadjuvant radiochemotherapy is the initial treatment, followed by surgery with curative intent.
The presentation at an early age is exceptional, as is the involvement of the seminal vesicles and the prostate.
When there is infiltration of the prostate and seminal vesicles, the surgery of choice is pelvic exenteration. But in some selected cases it is possible to perform en bloc resection surgery, preserving the sphincter apparatus and the bladder. This will result in a better quality of life for the patient without compromising the oncological prognosis.
The coloanal anastomosis can be performed at the same time and protected with an ostomy, or delayed through the pull through procedure
Description: We present the clinical case of a 24-year-old man, with a 3-month history of rectal bleeding, constipation, and pelvic pain.
Low rectal cancer with prostate-seminal infiltration without systemic leakage was diagnosed. Neoadjuvant therapy with radiochemotherapy was performed.
The tumor committee decided to perform a TaTME transsphincteric ultra-low anterior rectal resection plus laparoscopic en bloc resection of the prostate and seminal vesicles.
Patient in Lloyd Davies position, Trendelenburg 30º and lateralized to the right.
12 mmHg pneumoperitoneum with 12 mm supraumbilical optical trocar for the camera. Another 4 ports were placed, two of 12 mm on the flank and FID for the surgeon, and two of 5 mm on the flank and FII for the second assistant.
The left angle was mobilized by medial approach; a section of the IMV below the Pancreas, and the IMA at its origin. We completed the retrorectal dissection, and in front the anteroproximal sector of the seminal vesicles.
The transanal time began with the intersphincteric dissection until the anorectal ring was overcome, completing the TME by the video-assisted transanal route.
Simultaneously, the Urology team performed the prostatectomy and release of the seminal vesicles in block with the rectum, and making the vesico-urethral anastomosis.
The descending colon was exteriorized in the form of a Pull Through. At 10 days, the redundant colon was resected and the coloanal anastomosis was secured.
The patient had a postoperative period without complications, tolerating the oral route with a progressive diet, urinating without a catheter, and mobilizing the intestine. Discharge 14 days after the initial surgery. He was followed up at 15 and 30 days, being asymptomatic, with practically normal urinary continence. The perianal inspection revealed an anus with preserved mucocutaneous folds, and a somewhat hypotonic sphincter on rectal examination, which voluntarily contracted, achieving partial continence.
Conclusions: Locally advanced lower rectal cancer remains a therapeutic challenge.
Pelvic exenteration is the surgery of choice for genitourinary invasive rectal tumors. Sphincter and bladder preservation surgery emerges as a therapeutic possibility in strictly selected cases.
The Delayed Pull Through coloanal anastomosis has reappeared in recent years with the aim of reducing the need for detransitation stomas and suture failure.
Keywords: Rectal Cancer; Transsphincteric Ultra-low Anterior Resection; TaTME; Prostatectomy
REFERENCIAS