Complicated Meckel's diverticulum. Fifteen
years of experience
Complicated Meckel's diverticulum. Fifteen
years of experience
in an interzonal
hospital in the Province of Buenos Aires

Rocío Pérez Domínguez, Guillermina Candia, Hernán
Alejandro Santilli, Sergio Schlain
Hospital Interzonal General de Agudos San
Roque, Gonnet, Provincia de Buenos Aires
ABSTRACT
Introduction: Meckel's diverticulum is the most common congenital
malformation of the gastrointestinal tract. It can present with bleeding, intestinal obstruction or
diverticulitis, complications that decrease with age, so in adults the
diagnosis is usually incidental. Treatment of complications is surgical, through
diverticulectomy or segmental resection of the small intestine, depending on
its morphological characteristics.
Objective: to analyze our experience in the management of complicated
Meckel's diverticulum over a period of 15 years.
Design: descriptive, observational, cross-sectional, retrospective
study.
Materials and methods: the medical records of patients operated on for
complicated Meckel's diverticulum in the General Surgery Service of the San
Roque Hospital during the period 2007-2022 were reviewed. Demographic data,
clinical presentation, preoperative diagnosis, surgical treatment,
postoperative complications, and histopathological findings were recorded.
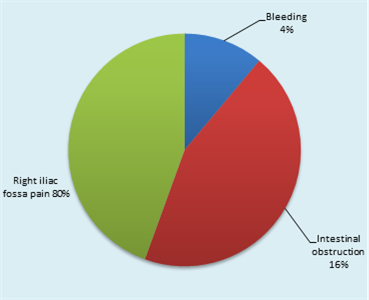
Results: twenty-five patients were included, 21 (84%) men, 3 under
18 years of age. The clinical presentation was a right iliac fossa syndrome
in 80% of cases, intestinal obstruction in 16% and hemorrhage in 4%. In only 2 cases was
the preoperative diagnosis made, confirmed by computed tomography. Diverticulectomy was
performed in 68% of patients and segmental resection in 32%. The approach was by
laparotomy in 64%, mainly in the initial period, and by laparoscopy in 36%. There was a
Clavien-Dindo IIIb complication in a pediatric patient treated with
percutaneous drainage. In only one patient (4%), who presented with massive
gastrointestinal bleeding, gastric-type epithelium and ectopic pancreas were
found in the diverticulum.
Conclusions: in our experience, complicated Meckel's diverticulum
occurred predominantly in men. The most frequent complication in adults was
diverticulitis. Preoperative diagnosis was infrequent and was made by
computed tomography. Diverticulectomy is sufficient in most cases. Currently, laparoscopy
is a safe, profitable and efficient tool that allows for the timely diagnosis
and treatment of this entity.
Keywords: Meckel's diverticulum, adult, abdominal pain,
diverticulitis, intestinal obstruction, intestinal bleeding, surgical treatment
INTRODUCTION
Meckel's diverticulum is the most common congenital
malformation of the gastrointestinal tract with an incidence of 0.3-2.9%.1 It
represents the incomplete involution of the omphalomesenteric duct that is
normally obliterated between the fifth and seventh week of intrauterine life. It
is usually asymptomatic or an intraoperative finding in surgeries for other
abdominal pathologies. It can present with symptoms of bleeding, intestinal
obstruction or diverticulitis, depending on age, which is why it is sometimes
called “the great pretender.” These complications decrease with age, so the
diagnosis of Meckel's diverticulum in adults is usually incidental. Although
only a low percentage of the adult population can suffer complications
throughout life, their consequences can be serious. For diagnosis, imaging
studies have low sensitivity and specificity, however, exploratory laparoscopy
is an important tool. Surgical treatment with resection of the diverticulum is
mandatory in the presence of complications, but remains debatable when they are
found incidentally. Intestinal resection followed by anastomosis appears
preferable to wedge resection or side-to-side stapled suturing because of the
risk of leaving abnormal heterotopic mucosa.
The objective of this presentation is to communicate the experience of 15 years
in an interzonal hospital in the Province of Buenos Aires.
MATERIAL
AND METHODS
A
descriptive, observational, retrospective, cross-sectional study was carried
out, analyzing the medical records of the General Surgery Service of the San
Roque Hospital during the period 2007-2022. All patients who presented with an
acute abdomen due to a complicated Meckel's diverticulum were included,
excluding those found incidentally.
RESULTS
Distribution by age and sex
Twenty-five
patients were included in the 15-year study period, 1.66 cases per year, with
an age range of 7 to 61 years. Twenty-one patients (84%) were men, 3 were
younger than 18 years of age, and 4 (16%) were women.
Clinical presentation
The
most frequent clinical presentation was right iliac fossa pain in 20 patients,
followed by intestinal obstruction in 4 and intestinal bleeding in 1 (Fig. 1).
Diagnostic methods
The
diagnosis of acute abdomen was carried out through physical examination and
complementary studies. Laboratory tests showed neutrophilia. Plain abdominal X-ray, performed in all patients, showed air-fluid
levels of the small intestine in patients who presented obstructive symptoms.
In 6 cases, abdominal ultrasound was performed, which
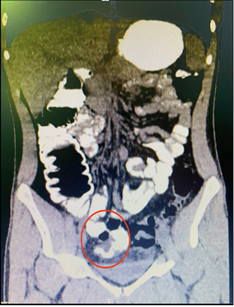
showed little free fluid in the right iliac fossa. Only in 2 patients with
suspected complicated Meckel's diverticulum, an abdominal CT scan was
requested, which certified the diagnosis. The first was a 67-year-old patient
who presented with central abdominal pain and vomiting for 2 days, with no
response to medical treatment. The CT scan showed the presence of a diverticular
sac with inflammatory characteristics dependent on the small intestine,
associated with marked air-fluid levels. The second corresponds to a
17-year-old man who attended the emergency room for episodes of hematochezia
lasting 36 hours, with hemodynamic compromise, in whom colonoscopy did not show
colonic bleeding. The CT scan showed a blind cul-de-sac arising from the small
intestine with contrast inside.
Surgical treatment
Sixty-eigth
percent (17) of the patients were treated by diverticulectomy (Fig. 3 A and B),
while the remaining 32 percent (8) underwent ileal resection with end-to-end
anastomosis (Fig. 3 C). The approach used was predominantly laparotomic (64%)
using a Mc Burney incision, mainly during the first years of the study, while
36% underwent laparoscopy.
Complications
A IIIb complication of the Clavien-Dindo classification
was recorded in a pediatric patient, who was referred for percutaneous
drainage. There was no associated mortality.
Histopathology
The diverticula had intestinal-type epithelium,
associated with vasocongestion and edema. Only 1 (4%) had gastric-type epithelium, formed by
polypoid projections and fundic glands in the lamina propria, and ectopic
pancreas. It corresponds to the patient who
presented massive intestinal bleeding. No malignant neoplasms were identified.
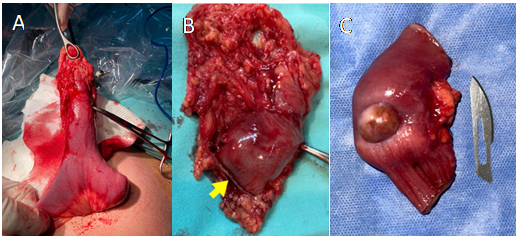
Figure 3. Surgical
treatment of different Meckel's diverticula. A.
Exteriorization of the small intestine with the presence of a diverticulum
more than 5
cm long on its antimesenteric border.
B.
Resection line after diverticulectomy
using an endostapler (arrow). C. Resection
of
the small
bowel segment that includes a diverticulum with a wide, indurated base.
DISCUSSION
Meckel's diverticulum was described for the first time
in an article published by the German anatomist Johann Friedrich Meckel in
1809. Its appearance is the same in men and women, although according to Park
et al.2 the incidence of complicated diverticula is higher in men
with a 3:1 ratio. In our series it was 5:1.
The
diverticulum is usually located on the antimesenteric border at an average
distance of 46 cm from the ileocecal valve and its average length is 3 to 5 cm.
It is made up of the three layers of the intestinal wall and its arterial
supply is through the superior mesenteric artery. It is lined mainly by typical
ileal mucosa, but because the yolk canal cells are pluripotent, other
heterotopic gastric (50%), pancreatic (5%) and, more rarely, hepatobiliary,
duodenal, colonic and endometrial tissues can be found.3
The
most common clinical presentation in adults is intestinal bleeding, which
occurs in 25-50% of patients, while intestinal obstruction predominates in
children under 2 years of age.
Intestinal
bleeding can be acute or chronic. The main mechanism of hemorrhage is acid
secretion from the ectopic mucosa, which leads to ulceration of the adjacent
ileal mucosa.
The
etiology of intestinal obstruction is diverse; may be due to a fibrous band
extending from the diverticulum to the umbilicus (14-53%), ulceration (<4%);
intussusception, Littre hernia or stenosis secondary to chronic diverticulitis.3,4
According to Sharma et al.,5 diverticulitis represents 20% of
symptomatic cases of Meckel's diverticulum, although in our series its
incidence was notably higher, reaching 80%. The pathophysiology is analogous to
that of acute appendicitis and the symptoms simulate this clinical picture, so
it should be considered the main differential diagnosis in those patients who
present pain in the right iliac fossa.
Preoperative diagnosis of Meckel's diverticulum remains
challenging. Ultrasound, X-ray,
angiography, CT scan or MRI can help in the diagnosis but the sensitivity and
specificity are low.5 However, they contribute by demonstrating the
presence of air-fluid levels suggestive of small bowel obstruction, or by
identifying a cecal appendix with normal characteristics, thus increasing the
suspicion of a complicated diverticulum. Exploration with labeled technetium-99
pertechnate is the most accurate non-invasive test to determine the presence of
Meckel's diverticulum due to the propensity of the tracer to concentrate in the
ectopic gastric mucosa.6 In children it has a sensitivity of 80-90%. a
specificity of 95% and an accuracy of 90%, but in adults it is less reliable,
with a sensitivity of 62.5%, a specificity of 9% and an accuracy of 46%.3
However, its availability in health centers, it is very limited.
In
this series, a preoperative diagnosis of complicated Meckel's diverticulum was
made in only two cases, confirmed by oral contrast-enhanced CT scan showing a
blind tubular structure arising from the small intestine.
The treatment of choice for symptomatic Meckel's diverticulum is surgical
resection. This can be achieved by diverticulectomy or by segmental intestinal
resection and anastomosis1. The extent of resection is determined based on
intraoperative findings and the characteristics of the omphalomesenteric
remnant. The external appearance criteria have been studied, concluding that
long diverticula can be eliminated by simple transverse resection with a
stapler since the presence of ectopic tissue is usually lodged at its distal
end, while in short diverticula it can occur in any area. Therefore, it is
recommended to evaluate the base; If it is narrow, without the presence of a
palpable mass within the lumen of the ileum, a simple wedge resection followed
by primary closure of the defect can be chosen. On the other hand, if the base
is wide, heterotopic tissue is palpable, or there are associated inflammatory
or ischemic alterations, resection of an ileal segment and subsequent
end-to-end anastomosis with manual suture or staples should be chosen.
Regarding the approach, open surgery has long been used as an effective method
to treat complicated Meckel's diverticulum. However, in the era of minimally
invasive surgery, laparoscopic management has become a very appropriate
diagnostic and therapeutic tool.7-11
CONCLUSIONS
In our experience, complicated Meckel's diverticulum
occurred predominantly in men. The most frequent complication in adults was
diverticulitis, so the most common presumptive diagnosis was acute
appendicitis. Preoperative diagnosis was infrequent and was performed
using CT scan.
In two thirds of the cases the
treatment was diverticulectomy. Currently, laparoscopy is a safe,
cost-effective and efficient tool that allows for timely diagnosis and
treatment.
All surgeons must keep this entity in mind when faced
with an atypical abdominal syndrome that could reveal a complication of the
diverticulum, or due to the possibility of its incidental finding during
surgery for another reason.
REFERENCES
1.
Hansen CC, Søreide K. Systematic
review of epidemiology, presentation, and management of Meckel's diverticulum
in the 21st century. Medicine (Baltimore). 2018; 97: e12154.
2.
Park JJ, Wolff BG, Tollefson MK,
Walsh EE, Larson DR. Meckel's diverticulum: the Mayo Clinic experience with
1476 patients (1950-2002). Ann Surg. 2005; 241: 529-33.
3.
Sagar J, Kumar V, Shah DK. Meckel's
diverticulum: a systematic review. JRSoc Med. 2006; 99: 501-5.
4.
Kuru, Serdar. Meckel's
diverticulum: clinical features, diagnosis and management. Rev Esp Enf Dig. 2018; 110: 726-32.
5.
Sharma RK, Jain VK. Emergency
surgery for Meckel's diverticulum. World J Emerg Surg. 13;3:27.
6.
Levy, A. Meckel's diverticulum:
radiologic features with pathologic correlation. RadioGraphics. 2004;
24:565-87.
7.
Martin JP, Connor PD, Charles K.
Meckel's diverticulum. Am Fam Physician. 2000; 61: 1037-42.
8.
Sanders, LE. Laparoscopic treatment
of Meckel's diverticulum. Surg Endosc. 1995; 9: 724-27.
9.
Chan KW, Lee KH, Mou JW, Cheung ST,
Tam YH. Laparoscopic management of complicated Meckel's diverticulum in
children: a 10-year review. Surg
Endosc. 2008; 22:1509-12.
10.
Hosn MA, Lakis M, Faraj W, Khoury
G, Diba S. Laparoscopic approach to symptomatic Meckel's diverticulum in
adults. JSLS. 2014; 18: e2014.00349.
11.
Parvanescu A, Bruzzi M,
Voron T et al. Complicated Meckel's
diverticulum: Presentation modes in adults. Medicine. 2018; Sep; 97(38): e12457.